Über den Autor

PD Dr. Tim Hilgenfeld
Department of Neuroradiology, Heidelberg University HospitalIm Neuenheimer Feld 400
69120 Heidelberg
Germany
+49 6221 56 7566
tim.hilgenfeld@med.uni-heidelberg.de
https://www.klinikum.uni-heidelberg.de/neurologische-klinik/neuroradiologie/behandlungsspektrum/dental-mrt
Co-Autoren
Alexander Juerchott, Ulrich Karl Deisenhofer, Johannes Krisam, Peter Rammelsberg, Sabine Heiland, Martin Bendszus, Franz Sebastian Schwindling
Accuracy of CBCT, dental MRI, and intraoral radiography for detecting peri-implant bone defects at single zirconia implants—an in vitro study
Thema
Introduction
Zirconia is an attractive implant material due to its tooth-like colour, and its osseointegration potential [1]. The available evidence of short term observational periods suggests promising survival rates [2]. For specific zirconia implants, however, marginal bone loss was remarkably high [3, 4]. Therefore, early detection of bone lesions around zirconia implants is as important as for titanium implants. Peri-implantitis is a long-term complication and occurs despite successful osseointegration after implant placement. Peri-implant diseases are the most frequent biological implant complications (reported range 1% to 47%) [5, 6]. Their clinical importance will even increase as the number of placed implants is consistently increasing [7]. It is decisive to identify peri-implantitis as early as possible because the lesions are more aggressive than in periodontitis. It was shown that the absence of treatment leads to rapid disease progression [8]. Therefore, studies comparing sensitivity and specificity of different imaging methods are important to identify the most promising technique for early detection of bone lesions at zirconia implants.
Intraoral radiography (IR) is currently recommended as the best method for analysing bone loss. However, it is difficult to assess the type of defect by use of intraoral radiography [9]. This is problematic, because the configuration of the defect might affect the clinical outcome of peri-implantitis therapy [10]. Previous studies, therefore, have evaluated the use of cone beam computed tomography (CBCT); however, the results for defect detection at titanium implants have been inconsistent. While the performance of CBCT was poor in cases of thin buccal bone [11], other studies yielded more favourable results [12–14].
Dental magnetic resonance imaging (dMRI) is a promising new diagnostic tool in dentistry [15] with potential fields of application in endodontics [16, 17], implantology [18], orthodontics [19] and periodontology [20]. Recently dMRI attracted attention for study of zirconia implants [21, 22], and excellent contrast and limited artefacts have been observed [18]. Because it is a radiation-free imaging method, high-resolution dMRI could be a valuable 3-dimensional imaging alternative to CBCT.
Problem
Bone lesion detection around zirconia implants has not been studied by use of either intraoral radiography (IR) or cone-beam computed tomography (CBCT). Zirconia implants generate significantly more artifacts in CBCT than titanium implants [23]. Consequently, study results from titanium implants cannot be applied to zirconia implants [24].
Aim
Our in vitro study compares the diagnostic accuracy and reliability of three imaging methods (IR, CBCT, and dMRI) at single zirconia implants for detection of peri-implant bone lesions and correct classification of the morphology of the lesions.
Materials
Fresh bovine ribs were cut into 48 bone specimens of 4 cm length. Two sizes of peri-implant lesions were created: small defects (1 mm in width and depth) and large defects (3 mm in width and depth). All 48 specimens received zirconia implants (Straumann PURE Ceramic Implant, 4.1 x 10 mm, Straumann Holding AG, Basel, Switzerland), in accordance with the manufacturer’s protocol. Subsequently, all 48 samples were randomly assigned to either the study group (n = 24, with peri-implant bone defects) or the control group (n = 24, no bone defects). In the study group, four defect morphologies were created, according to the classification of Renvert & Giovannoli [25]. The four defect types were: 1-wall-(w), 2-w-, 3-w- and 4-w-defects. Each defect type was produced in both defect sizes at three specimens (resulting in n = 24 samples). Acid etching was applied to simulate a realistic surface of the peri-implant bone defects. After implant placement, the bone defects were filled and covered with a fresh bovine muscle graft to simulate soft tissues (Fig. 1). Previous publications studying infected implants in other body regions reported even higher signal intensities of infected soft tissue compared to non-affected muscle tissue e.g. by soft tissue edema or fluid collections [26, 27]. Therefore, our method will not artificially overestimate the diagnostic accuracy of dMRI.
Imaging was performed using a Heliodent DS (Dentsply Sirona; 60 kV, 7 mA and 0.08 s), a 3D Accuitomo 170 (J Morita; field of view: 4 x 4 cm2, 90 kV, 7 mA, rotation of 360° and a voxel size of 80 µm) and a 3T MRI-system (Magnetom-TIM-Trio; Siemens Healthcare GmbH) by use of two standard small 4-Channel Flex Coils (Siemens Healthcare GmbH). The MSVAT-SPACE prototype sequence was specially optimised and evaluated for high-resolution dMRI, as described elsewhere [28]. Altogether 144 IR-, dMRI- and CBCT-datasets were anonymised, exported as DICOM and analysed by two radiologists and two dentists. They were blinded and repeated the analysis after two weeks. For each dataset, the readers selected among five of the following answers: I. no defect visible; II. 1w defect; III. 2w defect; IV. 3w defect; V. 4w defect. Cohen’s and Fleiss’ Kappa (κ) and the 95 % confidence interval (CI) were used to analyse intra- and inter-reader agreement of defect detection, defect morphology and defect size for each modality. Sensitivity, specificity and likelihood ratios (LR+ and LK-) were calculated for each defect size, defect type and modality to determine the diagnostic accuracy.
Results
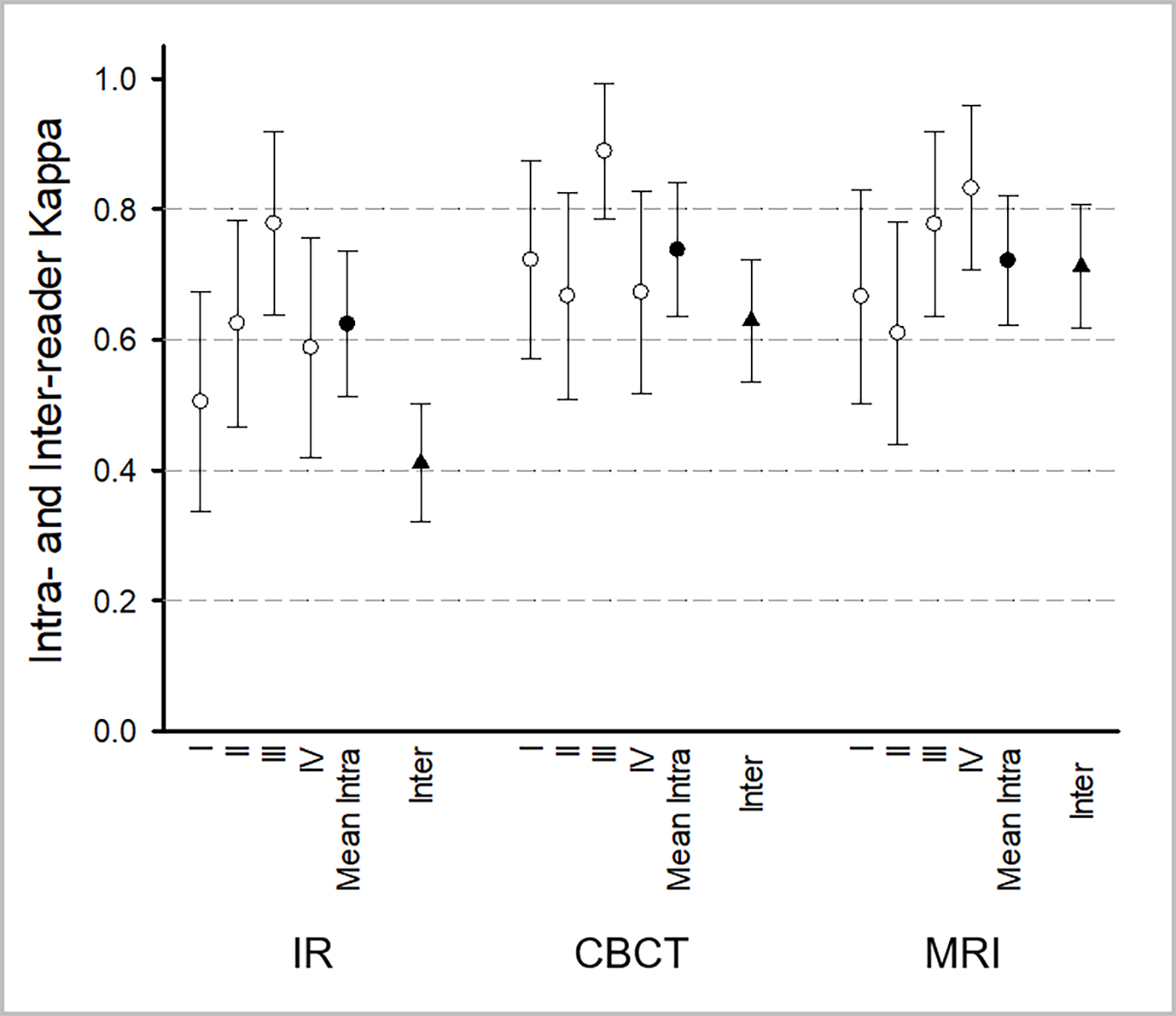
All three modalities revealed a high reliability (κ range: 0.832-1). κ-values were higher for CBCT and dMRI than for IR. Furthermore, mean intra-reader agreement and the Fleiss’ Kappa measuring the inter-reader agreement between all four readers of CBCT and dMRI were higher than for IR (Fig. 2).
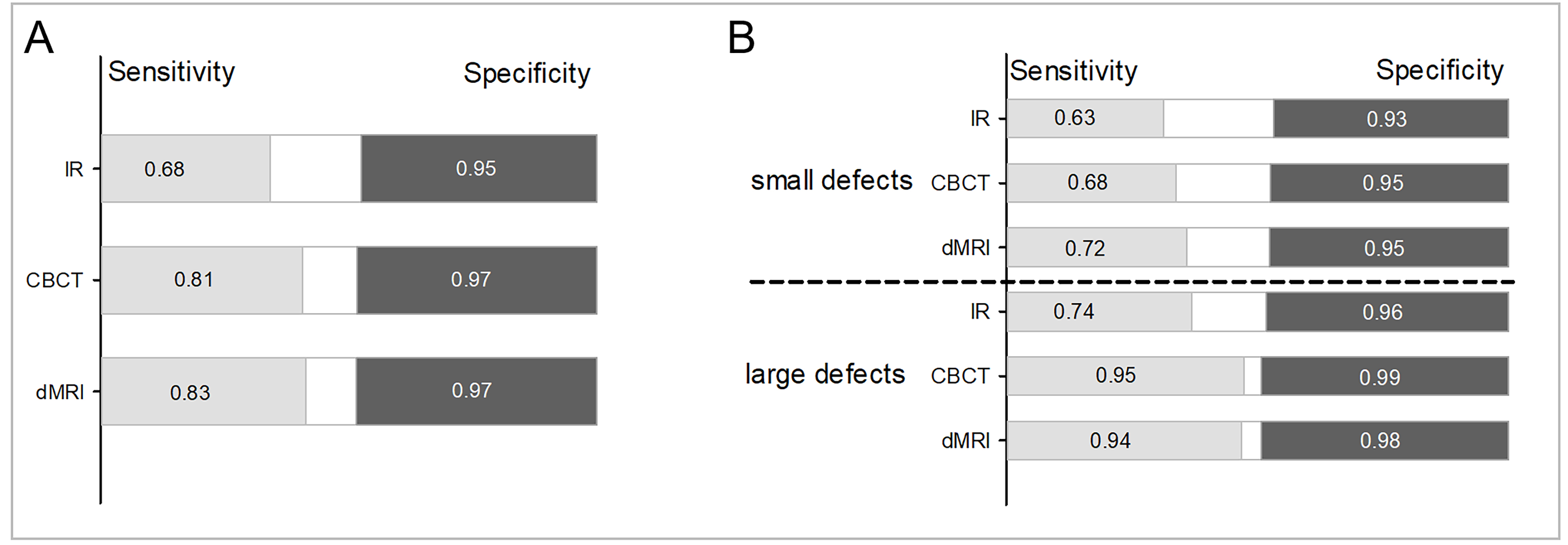
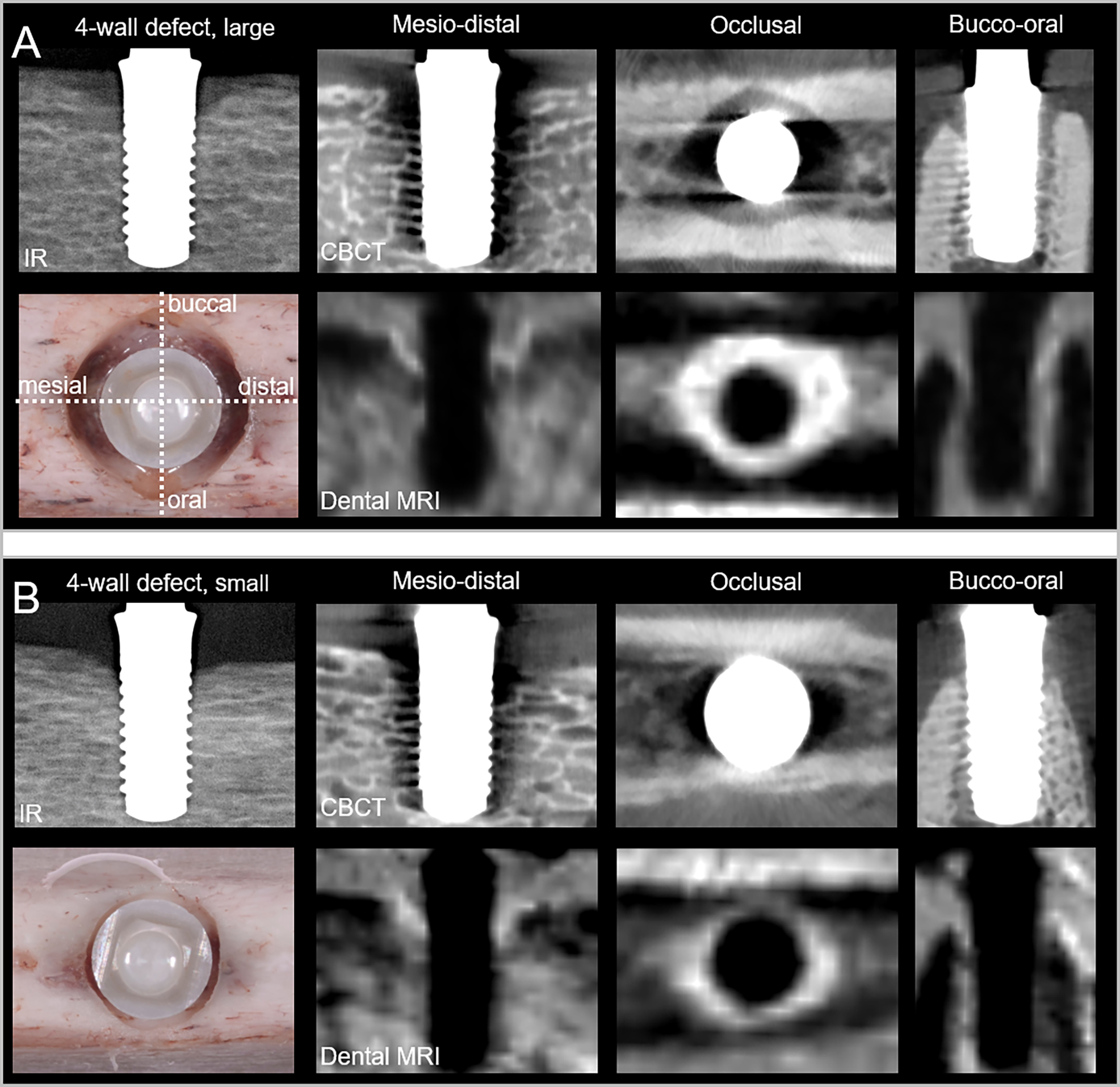
All readers correctly identified nearly all defects and all controls for CBCT (sensitivity: 0.99; specificity: 1) and dMRI (sensitivity: 1; specificity: 0.99). Sensitivity and specificity were also high for IR (0.97; 0.96), but significantly different from those for CBCT (p = 0.006) and dMRI (p = 0.003). Sensitivity for correct detection of defect type was highest for dMRI (0.83; Fig. 3A), closely followed by CBCT (0.81), with no statistically significant difference (p = 1; typical images are given in Fig. 4). The lowest sensitivity was recorded for IR (0.68). The IR results were significantly different from those for CBCT (p = 0.003) and dMRI (p = 0.004). The respective specificity values were comparable for all three methods (range: 0.95–0.97; Fig. 3A). In a second step, a sub-analysis for correct detection and defect type classification of small and large defects was performed. Only minor, non-significant differences were found between sensitivity of CBCT and dMRI for classification of small (0.68 vs. 0.72) and large (0.95 vs. 0.94) defects (Fig. 3B). However, the sensitivity of IR was lower for both defect sizes (small: 0.63; large: 0.74; Fig. 3B). CBCT and dMRI results differed significantly from IR results for large defects (CBCT vs. IR: p = 0.0001; dMRI vs. IR: p = 0.003), but not for small defects.
In a third step, a sub-analysis of each defect type was performed. For detection of small 1w defects, IR (0.88) outperformed CBCT (0.79) and dMRI (0.71; Table 2; Fig. 5). For most defects, however, sensitivity was higher for CBCT and dMRI than for IR, with the greatest difference for large 4w defects (IR / CBCT / dMRI: 0.42 / 1 / 0.96; example images are given in Figure 6). Regarding small 4w defects dMRI (0.67) outperformed IR (0.33) and CBCT (0.33). Overall, only minor differences in specificity were found between the three imaging methods.
Discussion
Within the limitations of an in vitro study, our results emphasize the usefulness of IR, CBCT, and dMRI for detection/exclusion of peri-implant bone defects at zirconia implants. However, differences were noted when classifying different defect types. Significantly higher sensitivity and better inter-reader reliability were observed for CBCT and dMRI than for IR. This sensitivity advantage of CBCT and dMRI in defect classification depended on lesion size; No significant differences in sensitivity were noted for the group of small defects. In contrast, CBCT and dMRI performed significantly better than IR for large defects. No significant difference was observed between dMRI and CBCT.
As far as the authors are aware, this is the first study to assess radiation-free dMRI for evaluation of peri-implant bone defects. Sensitivity and specificity of dMRI and CBCT were comparable. Advanced artefact-suppression techniques resulted in improved visibility of bone defects in dMRI compared to CBCT (Fig. 6). Therefore, dMRI is a promising tool for future in vivo studies on bone defects at zirconia implants.
It is still under debate whether the peri-implant defect configuration affects therapy outcome [29]. Most authors, however, believe it does, thus emphasizing the clinical relevance of our findings [10, 30–33]. In addition, identification of the most common peri-implant bone defect in humans—the 4w defect [34] —was much better for CBCT and dMRI than for IR for the large defect type. For small 4w defects, dMRI outperformed CBCT and IR. This is interesting, as this specific defect seems to benefit from surgical regenerative therapy [10]. Surprisingly, sensitivity for detection of peri-implant bone defects was comparable for CBCT and IR, but sensitivity for classification of defects was greater for CBCT than for IR. Because intense beam-hardening artifacts for zirconia implants have been observed in previous studies, and were more severe than for titanium implants [23], poorer results were expected. Nevertheless, the bone defects were visible in at least some areas around every implant, because artefacts were limited to specific regions. This has been similarly described for titanium implants [35].
Other authors have previously assessed the accuracy of IR and CBCT for defect classification at titanium implants. They reported comparable sensitivity for IR and CBCT. Dave et al. recorded high sensitivity of IR (1) and CBCT (0.98) for detection of 0.675 mm bone defects [36].
Our study has some limitations that must be acknowledged. First, an in vitro model with standardised defects was used, and defects were created artificially. Moreover, sensitivity and specificity of CBCT and dMRI artefacts may be reduced in vivo. Because of the vicinity of peri-implant bone defects and crowns, beam hardening and extinction artifacts due to metallic restorations, even from the contralateral side, will reduce the defect visibility in CBCT images. Furthermore, metallic restorations adjacent to the implant will affect the defect visibility in dMRI as well. Our study demonstrates the need for prospective in vivo studies to further investigate the significance of IR, CBCT, and dMRI for peri-implant defect detection.
Conclusion
Within the limitations of an in vitro study, our results emphasize the usefulness of IR as the standard imaging method for detection of peri-implant bone defects at single zirconia implants. Our data also indicate that CBCT and dMRI may be advantageous for defect classification. However, they cannot be recommended as first imaging methods given the higher radiation dose and cost of CBCT, and the experimental character of dMRI.
Bildergalerie (6)



Literatur:
- Pieralli, S., et al., Osseointegration of zirconia dental implants in animal investigations: A systematic review and meta-analysis. Dent Mater, 2017.
- Pieralli, S., et al., Clinical Outcomes of Zirconia Dental Implants: A Systematic Review. J Dent Res, 2017. 96(1): p. 38-46.
- Kohal, R.J., et al., One-piece zirconia oral implants for single-tooth replacement: Three-year results from a long-term prospective cohort study. J Clin Periodontol, 2017.
- Kohal, R.J., et al., Peri-implant bone response to retrieved human zirconia oral implants after a 4-year loading period: A histologic and histomorphometric evaluation of 22 cases. J Biomed Mater Res B Appl Biomater, 2016. 104(8): p. 1622-1631.
- Tarnow, D.P., Increasing Prevalence of Peri-implantitis. Journal of Dental Research, 2016. 95(1): p. 7-8.
- Derks, J. and C. Tomasi, Peri‐implant health and disease. A systematic review of current epidemiology. Journal of Clinical Periodontology, 2015. 42(S16).
- Jordan, R.A., et al., Fifth German Oral health study. 1 ed. 2016: Deutscher Ärzte Verlag.
- Salvi, G.E., R. Cosgarea, and A. Sculean, Prevalence and Mechanisms of Peri-implant Diseases. Journal of Dental Research, 2017. 96(1): p. 31-37.
- Kühl, S., et al., Detection of peri-implant bone defects with different radiographic techniques - a human cadaver study. Clin Oral Implants Res, 2016. 27(5): p. 529-34.
- Schwarz, F., et al., Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol, 2010. 37(5): p. 449-55.
- Fienitz, T., et al., Accuracy of cone beam computed tomography in assessing peri-implant bone defect regeneration: a histologically controlled study in dogs. Clin Oral Implants Res, 2012. 23(7): p. 882-7.
- Ritter, L., et al., Accuracy of peri-implant bone evaluation using cone beam CT, digital intra-oral radiographs and histology. Dentomaxillofac Radiol, 2014. 43(6): p. 20130088.
- Bohner, L.O.L., et al., Comparative analysis of imaging techniques for diagnostic accuracy of peri-implant bone defects: a meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol, 2017. 124(4): p. 432-440 e5.
- Kamburoglu, K., et al., Accuracy of CBCT images in the assessment of buccal marginal alveolar peri-implant defects: effect of field of view. Dentomaxillofac Radiol, 2014. 43(4): p. 20130332.
- Di Nardo, D., et al., Nuclear Magnetic Resonance Imaging in Endodontics: A Review. Journal of endodontics, 2018.
- Iohara, K., et al., Assessment of Pulp Regeneration Induced by Stem Cell Therapy by Magnetic Resonance Imaging. Journal of Endodontics, 2016. 42(3): p. 397-401.
- Juerchott, A., et al., Differentiation of periapical granulomas and cysts by using dental MRI: a pilot study. International journal of oral science, 2018: p. 17.
- Duttenhoefer, F., et al., Magnetic resonance imaging in zirconia-based dental implantology. Clin Oral Implants Res, 2015. 26(10): p. 1195-202.
- Heil, A., et al., Lateral cephalometric analysis for treatment planning in orthodontics based on MRI compared with radiographs: A feasibility study in children and adolescents. PLoS One, 2017. 12(3): p. e0174524.
- Hilgenfeld, T., et al., High-resolution dental magnetic resonance imaging for planning palatal graft surgery-a clinical pilot study. J Clin Periodontol, 2018. 45(4): p. 462-470.
- Hilgenfeld, T., et al., Artefacts of implant-supported single crowns - Impact of material composition on artefact volume on dental MRI. Eur J Oral Implantol, 2016. 9(3): p. 301-308.
- Benic, G.I., M. Elmasry, and C.H. Hämmerle, Novel digital imaging techniques to assess the outcome in oral rehabilitation with dental implants: a narrative review. Clin Oral Implants Res, 2015. 26 Suppl 11: p. 86-96.
- Sancho-Puchades, M., C.H. Hämmerle, and G.I. Benic, In vitro assessment of artifacts induced by titanium, titanium-zirconium and zirconium dioxide implants in cone-beam computed tomography. Clin Oral Implants Res, 2015. 26(10): p. 1222-8.
- Liedke, G.S., et al., Factors affecting the possibility to detect buccal bone condition around dental implants using cone beam computed tomography. Clin Oral Implants Res, 2017. 28(9): p. 1082-1088.
- Renvert, S. and J.L. Giovannoli, Peri-implantitis. Vol. 1. 2012: Quintessence Publishing. 272.
- Hayter, C.L., M.F. Koff, and H.G. Potter, Magnetic resonance imaging of the postoperative hip. Journal of Magnetic Resonance Imaging, 2012. 35(5): p. 1013-1025.
- Plodkowski, A.J., et al., Lamellated Hyperintense Synovitis: Potential MR Imaging Sign of an Infected Knee Arthroplasty. Radiology, 2013. 266(1): p. 256-260.
- Hilgenfeld, T., et al., PETRA, MSVAT-SPACE and SEMAC sequences for metal artefact reduction in dental MR imaging. Eur Radiol, 2017. 27(12): p. 5104-5112.
- Roccuzzo, M., et al., Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen. J Clin Periodontol, 2016. 43(3): p. 311-8.
- Ding, Q., et al., Association Between Peri-implant Bone Morphology and Marginal Bone Loss: A Retrospective Study on Implant-Supported Mandibular Overdentures. Int J Oral Maxillofac Implants, 2017. 32(1): p. 147-155.
- Khoshkam, V., et al., Reconstructive procedures for treating peri-implantitis: a systematic review. J Dent Res, 2013. 92(12 Suppl): p. 131S-8S.
- Tarnow, D.P., S.J. Chu, and P.D. Fletcher, Clinical Decisions: Determining When to Save or Remove an Ailing Implant. Compend Contin Educ Dent, 2016. 37(4): p. 233-243;quiz244.
- Botticelli, D., T. Berglundh, and J. Lindhe, Resolution of bone defects of varying dimension and configuration in the marginal portion of the peri-implant bone. An experimental study in the dog. J Clin Periodontol, 2004. 31(4): p. 309-17.
- Schwarz, F., et al., Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. Clin Oral Implants Res, 2007. 18(2): p. 161-70.
- Benic, G.I., et al., In vitro assessment of artifacts induced by titanium dental implants in cone beam computed tomography. Clin Oral Implants Res, 2013. 24(4): p. 378-83.
- Dave, M., et al., A comparison of cone beam computed tomography and conventional periapical radiography at detecting peri-implant bone defects. Clin Oral Implants Res, 2013. 24(6): p. 671-8.