Über den Autor

Dr. Daniel Ferrari, M.Sc.
Zahnarztpraxis Dr. Ferrari & KollegenHeinrichstraße 83-85
40239 Düsseldorf
Germany
0211-9083381
ferrari@zahnaerzte-heinrichstrasse.de
http://www.zahnaerzte-heinrichstrasse.de
Co-Autoren
D. Rothamel, D. Horvath, C. Klemm, U. Behrens, T. Fienitz, J.E. Zoeller
Callus distraction using HA-coated titanium plates
Thema
Background
The principle of distraction osteogenesis is based on the separation of a vital bone segment and consecutive expansion of an initial callus formed in between the mobile segment and the adjacent bone. In between a titanium surface and the surrounding bone a callus is also formed, if the titanium is placed in a sufficient distance to the bone surface (known as „jumping gap regeneration“ in immediate implant placement). Thus, a callus formed in between a titanium plate and the adjacent bone, might be also stable enough to be used for distraction osteogenesis, omitting the separation and fixation of a crestal bone segment.
Aim
The aim of the present pilot study is to evaluate the eligibility of a new minimally invasive distraction technique for vertical bone augmentation, based on the insertion and elevation of a thin HA-coated titanium plate and subsequent callus distraction underneath the titanium.
Material and Methods
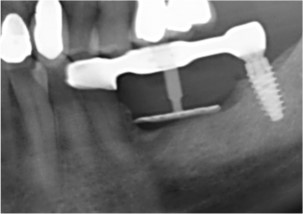
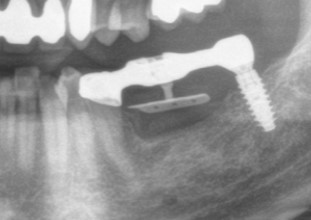
After approval of the clinical trial with a medical device by the local ethics committee of the University Hospital Cologne, Germany, and authorisation by the Federal Institute for Drugs and Medical Devices (BfArM; Bonn, Germany), six healthy patients revealing a vertical bone defect of the posterior maxilla or mandible (two bilateral) were consecutively included in the study. After mucoperiosteal flap elevation, HA-coated titanium plates (CelGen AG, Switzerland) were inserted with 1–2 mm distance to the underlying bone and fixed on the adjacent teeth using an individual bridge (Figs. 1–4). Soft tissue was thickened up underneath the periosteum using a 1 mm collagen matrix (mucoderm, botiss biomaterials, Germany; Fig. 5) and soft tissue was closed using single and mattress sutures. After a callus-forming phase of seven to ten days, membranes were elevated 0.7 mm per day until the individual desired augmentation heights of 4–8 mm were reached (Figs. 6 & 7). After a consolidation time of four to eight months, titanium plates were removed and bone core biopsies were harvested in progress of implant bed preparation (Figs. 8–12). Conventional radiographs were taken at baseline, before and after implant placement.
Results
Initial healing period was uneventful in all cases. Six of eight augmented areas showed sufficient vertical bone formation at the end of the consolidation period. Implants could be placed as planned before (Figs. 12–15), and histological evaluation showed excellent bone formation with physiological microarchitecture of the bone trephines and direct contact of bone to the titanium plates (Figs. 16–19).
After two months, one site revealed an inflammation-free complete reduction of the initially achieved augmentation height based on an insufficient retention of the titanium plate. One case showed a trauma-related soft tissue perforation after six weeks with consecutive removal of the device. Both cases are related to patient specific circumstances only.
In the other cases, radiographs taken after a consolidation period of four months showed initial mineralisation of the augmented area, increasing its radiodensity up to eight months. At implant uncovering, bone levels remained stable radiologically and clinically in both vertical and horizontal dimensions (Fig. 15).
Conclusions and clinical implications
Within the limits of the present pilot study it was concluded that this new technique of distraction osteogenesis using a HA-coated titanium plate in distance to the underlying bone supports predictable vertical bone regeneration in man (Proof of Concept). It is capable of representing a minimal invasive alternative for vertical ridge augmentation in the severely resorbed jaw. Currently, the parallel inclusion of a higher number of patients in a multicentre setting has just started to gain more data about the opportunities of this new bone regeneration device.
Just recently, a new and implant-supported internal distraction device (Bonehill, CelGen AG) allowing for even more minimal-invasive treatment (Figs. 20–25) has been included in the clinical study.
Bildergalerie (25)